Are Mental Institutions Coming Back?
The US Governments pivot on disabled rights and protections

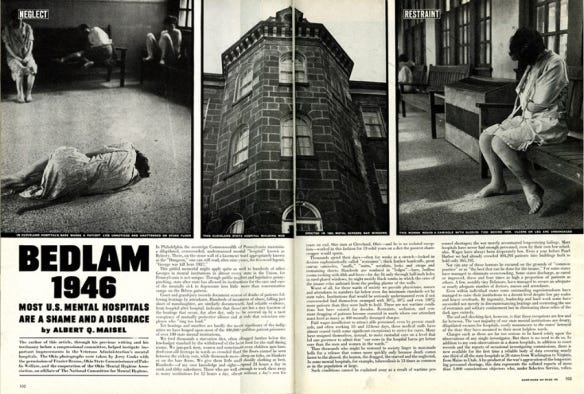
On May 6, 1946, Life magazine published photographs of an American psychiatric hospital that were so disturbing — so raw, so clearly damning — that readers compared them to the Nazi concentration camp documentation they had seen just weeks before. And that was a fair comparison. Journalist Albert Maisel documented that at the Philadelphia State Hospital at Byberry, more than 6,100 patients were packed into facilities built for a fraction of that number, supervised by just 180 attendants. Sixteen percent of the minimum staffing standard. Patients slept on bare floors, ate starvation rations, and were beaten by overworked staff who, as Maisel wrote, were “only the extreme end product” of a system built on contempt. He titled the piece “Bedlam.” From Bethlem Royal Hospital in London — a sixteenth-century institution so infamous for cruelty that its name became a synonym for chaos and horror. Maisel argued that, in three hundred years, the American version had not meaningfully improved.
In 2026, the federal government is building the conditions for a return to Byberry. To understand how we got here, it’s important to review the policies and systems that created and later attempted to address such environments. They don’t have whips and bare floors (yet), but with five policy decisions—each arguably defensible on its own, yet catastrophic together. At the end of this pipeline awaits a private, for-profit psychiatric facility billing Medicaid to institutionalize the disabled.
History First
The institutions of the twentieth century were not created in malice or to be abusive. Real reformers like Dorothea Dix campaigned in the 1840s to move mentally ill people OUT of prisons and poorhouses and INTO purpose-built hospitals where they might receive humane care. She was trying to care for the most vulnerable. The intent was real. What happened across the next century of underfunding, overcrowding, and institutional neglect was something else.
By the 1950s, more than 550,000 Americans lived in state psychiatric hospitals. They had been placed there sometimes voluntarily, more often not, because society had no other answer for them. Once placed, most of them stayed.
One example is Willowbrook State School on Staten Island that ran from 1956 to 1987. Willowbrook was the largest state-run institution for people with intellectual disabilities in the United States. It was also the site of one of the most egregious medical ethics violations in American history.
Between 1956 and 1971, a team of NYU researchers led by Dr. Saul Krugman deliberately infected children at Willowbrook with the hepatitis virus to study transmission. These children, who could not give consent, had developmental disabilities. Their parents were coerced by telling them the only available beds for their children were in the experimental ward, so if they could not afford care at home, they had the choice to enroll their child in experiments or have nowhere else to go.
The experiments ran for FIFTEEN years.
Outside the research ward: children lying unclothed on bare floors in their own waste. The children had no education, stimulation, no meaningful human contact. Senator Robert F. Kennedy toured the facility in 1965 and called it a “snake pit. In 1972, a young reporter named Geraldo Rivera got a camera and walked onto the grounds of Willowbrook. His ABC documentary showed America what its institutions actually looked like. A class-action lawsuit was filed that year. A federal consent decree in 1975 mandated phased closure. Willowbrook finally shut in 1987. Thirty-one years after the experiments began.
Willowbrook was not unusual. Pennhurst State School in Pennsylvania — documented in a 1968 television exposé called “Suffer the Little Children” — was found by a federal court to have subjected residents, many of them children, to abuse, neglect, and sexual assault in what the court called “inhumane” conditions. These conditions and treatments sound a lot like those in our ICE facilities now. In Alabama, Wyatt v. Stickney, filed in 1971, produced the first federal ruling that people involuntarily committed to state institutions have a constitutional right to actual treatment — not warehousing, but care with a realistic opportunity to return to society. That case ran for more than thirty years. It remains the longest mental health lawsuit in U.S. history.
The legal reckoning of the 1970s produced the deinstitutionalization movement, closing large state facilities and replacing them with community-based mental health centers, group homes, and supported living arrangements. The movement was backed by new psychotropic medications, genuine humanitarian principles, and the Mental Health Systems Act of 1980.
But Then Came Ronald Reagan… of course.
Ronald Reagan repealed the Mental Health Systems Act nine months after it passed. Deinstitutionalization continued, but the community infrastructure it was supposed to fund never materialized. People left institutions and entered communities that hadn’t been built to receive them. For many, it wasn’t liberation. It was a different kind of abandonment: the street, the criminal justice system, smaller private facilities with less oversight and the same capacity for neglect. Community integration only works when it is actively funded AND legally enforced. Without both, the institution in one form or another comes back.
Congress understood this in 1965. When it created Medicaid, it built in the Institution for Mental Diseases exclusion, which was a deliberate prohibition on using federal Medicaid funds to pay for care in large psychiatric facilities. To prevent facilities from trapping people in institutions that leadership had no intention of releasing them from, to profit off of them. It was a firewall.
The Case That Built the Floor
Lois Curtis and Elaine Wilson — L.C. and E.W. in court records — were two women with mental disabilities living in Georgia in the 1990s. Both had been voluntarily admitted to a state psychiatric institution. Both were later evaluated by their own treatment teams and cleared for community-based care. Both wanted to leave and were encouraged by their providers to go. Georgia refused to release them. Not because they were a danger or needed inpatient care but because community placement required resources the state hadn’t allocated, and institutionalization was cheaper to administer.
They sued under Title II of the Americans with Disabilities Act. In June 1999, the Supreme Court ruled six to three in their favor. Justice Ruth Bader Ginsburg wrote the majority, and her reasoning was direct: “Unjustified isolation is properly regarded as discrimination based on disability.” States are required to provide community-based services when the person wants them and when placement can be reasonably accommodated.
The ruling established what’s called the integration mandate — a legal requirement that disabled people be served in the most integrated setting appropriate to their needs. It forced every state to develop transition plans. It was, for millions of Americans with disabilities, the legal floor beneath their lives. To protect them from being isolated and institutionalized indiscriminately.
Into the Present
The current United States Government has declared it does not agree with this legal requirement and that people with disabilities do NOT have the right to be in integrated settings.In early 2026, the Department of Justice issued guidance signaling a retreat from the federal government’s longstanding interpretation of Olmstead. The DOJ had historically held that states had an affirmative obligation to plan for and fund community-based alternatives to institutionalization. The new guidance weakened that obligation, giving states broader discretion in determining what “reasonable accommodation” requires.
States facing budget pressure now have less legal risk when they cut home health aides, outpatient mental health services, and supported employment programs — the exact infrastructure that allows disabled people to stay out of institutions. Without active DOJ enforcement, the integration mandate is a right with no teeth. But this decision wasn’t made in isolation.
Attacks on Medicaid
On July 4, 2025, President Trump signed H.R. 1 — the “One Big Beautiful Bill Act.” Buried in its Medicaid provisions: adults 18 to 65 must demonstrate at least 20 hours per week of work, job training, or community service or lose coverage. Medical exemptions exist on paper, but claiming them requires documentation, case management navigation, and bureaucratic follow-through that an enormous number of disabled people — particularly those with serious mental illness, cognitive disabilities, or unstable housing — cannot reliably complete.
The Congressional Budget Office estimates H.R. 1’s Medicaid provisions will cut federal spending by $326 billion over ten years and cause millions to lose coverage. NPR reported in June 2026 that people with HIV, cancer, and serious mental illness, who technically qualify for exemptions, are already losing coverage because they cannot navigate the paperwork in time.
Here is the structural cruelty: Medicaid doesn’t merely cover doctor visits. For many disabled Americans, Medicaid funds the home health aides, behavioral health services, prescription medications, and supported employment programs that make working possible in the first place. The work requirement removes the scaffolding and then penalizes people for falling.
If you lose Medicaid, then you go into debt with medical costs and are more likely to lose any work you do have. But they are also coming after housing.
The Housing Floor Disappears
Disabled Americans are disproportionately represented among Section 8 housing voucher recipients. Disability is associated with reduced earning capacity, increased medical expenses, and heightened vulnerability to economic shocks. For hundreds of thousands of disabled people, a Section 8 voucher is the only thing between them and no address.
The Trump administration’s FY2026 budget proposed cutting HUD’s rental assistance programs by approximately 43 percent — $26.7 billion — and converting Section 8 into a block grant program in which states set eligibility rules. Congress did not pass the full 40 percent cut. But neither chamber fully funded voucher renewals. Under the House bill, 181,900 households lose rental assistance. Under the Senate plan, 107,800 lose theirs. Housing authorities across the country are already notifying recipients. The cuts are already here, and a larger percentage of the cuts that will hurt Americans land after midterms.
Lose the healthcare. Lose the job. Lose the home.
Survival Becomes Criminal
In June 2024, the Supreme Court ruled in City of Grants Pass v. Johnson that cities may enforce anti-camping ordinances against unhoused people even when no shelter is available. It overturned a Ninth Circuit decision that had held: criminalizing survival behavior when there is literally no alternative is cruel and unusual punishment.
Since that ruling, cities have enacted or re-enacted ordinances making it a criminal offense to sleep outside, to sit on sidewalks, to camp on public land. Enforcement falls disproportionately on people with mental illness, substance use disorders, and cognitive disabilities. These are the exact same people most dependent on community-based mental health services that are simultaneously being gutted.
A disabled person — unmedicated because they lost Medicaid, outside because they lost their voucher, unable to access a shelter that can’t accommodate their needs — is now a criminal by definition.
The arrest is the threshold. What comes after is where we follow the money.
Footing the Bill
The Institution for Mental Diseases (IMD) exclusion has, since 1965, prohibited Medicaid from paying for care in psychiatric facilities with more than 16 beds for adults 21 to 64. Congress built that firewall knowing exactly what it was preventing. They knew what happened when financial incentives and institutional capacity intersected without restriction or oversight. And there were exceptions via Section 1115 waivers. These waivers were state exemptions allowing Medicaid to pay for short-term stays in large psychiatric facilities. As of mid-2025, sixteen states hold mental health waivers. Thirty-seven hold substance use disorder waivers.
Before his Senate confirmation as Secretary of Health and Human Services, Robert F. Kennedy Jr. called explicitly for Congress to lift the exclusion nationwide. The Manhattan Institute and the American Enterprise Institute have published the intellectual case for full repeal, framing it as mental health reform.
Now there are genuine arguments that short-term inpatient care can be beneficial, also valid arguments that Medicaid should be used for long term care. I absolutely support those on Medicaid getting treatment for substance abuse or mental health treatment. But EVERY SINGLE ONE of those arguments is missing a reckoning with what happens when full repeal of the exclusion is combined with the simultaneous demolition of the community-based alternatives that were supposed to prevent anyone from needing those facilities in the first place. And RFK Jr. isn’t calling for repeal out of the goodness of his heart but for money, of course.
A person who has lost their Medicaid, their employment supports, their housing, been arrested under a Grants Pass ordinance, and been involuntarily committed is placed in a private, for-profit psychiatric facility. Without the exclusion, the institution bills Medicaid for the stay. The institution is now being paid by the same federal program that just cut this person off. The money that was deemed too expensive to keep someone housed and medicated in their community becomes, after arrest and commitment, a billable event. Private institutions get to make money off of everyone they house, for as long as they house them, from the same program that could have kept them home with their families and friends.
The Reality
The last patient left Willowbrook in 1987. Thirty-nine years ago. People who were held there are alive today. The infrastructure of abuse that those cases dismantled over 30 years of litigation, legislative action, and federal enforcement was not some pre-modern horror. It was recent. It was documented. It was legal.
And the specific conditions that enabled it, such as institutional financial incentives, inadequate community alternatives, unenforced legal protections, poverty that leaves disabled people with no margin for error — are being reconstructed under “reform” and “fiscal responsibility”. How much did we just spend on the war with Iran?
The IMD exclusion stood for sixty years because Congress understood what had come before it. Financial incentives, for-profit imprisonment and institutionalization, if left unchecked, lead to the abuse of the vulnerable. Disabled people have the right to live in their communities as much as possible. Medicaid should cover a parent being a caregiver, not an institution housing them against their (or their family’s) wishes. Removing the IMD exclusion should only be considered with full funding and enforcement of the Olmstead decision and community care guidelines.
In 1999, the Supreme Court said: you have the right to a life in your community. In the US, we have the money; we just have the wrong priorities. And who is going to build and own these institutions? What “friend” is going to profit off it? In 2026, the federal government is making that right impossible to exercise, and building, piece by piece, the infrastructure to hold the disabled indefinitely when it fails.
L.C. and E.W. won their case. The question is whether we let the conditions that made it necessary come back. At the moment, we are.
Sources:
Scholastica: Willowbrook, Institutional Abuse, and Disability Rights
Work Requirements in the 2025 Federal Budget Reconciliation Law – KFF
Work Requirements Comparison After P.L. 119-21 – Congress.gov
Strict Medicaid Work Rules Could Harm People With Serious Illnesses – NPR
Medicaid’s IMD Exclusion: The Case for Repeal – Manhattan Institute
E. Fuller Torrey, The Insanity Offense (2008); NAMI historical data — peak U.S. state psychiatric hospital population, 1955 (~558,000)
Albert Maisel, “Bedlam 1946,” Life magazine, May 6, 1946 — conditions at Byberry and Cleveland State Hospital
Willowbrook hepatitis experiments, 1956–1971 — Dr. Saul Krugman, NYU; coerced parental consent via admission access
Geraldo Rivera documentary, ABC, 1972; Willowbrook class-action lawsuit; federal consent decree 1975; school closed 1987
Halderman v. Pennhurst State School & Hospital; “Suffer the Little Children” (1968 TV exposé)
Wyatt v. Stickney, M.D. Ala. 1972 — first federal ruling establishing constitutional right to treatment; 30+ years of litigation
Olmstead v. L.C., 527 U.S. 581 (1999) — majority opinion by Justice Ruth Bader Ginsburg
DOJ guidance retreating from Olmstead enforcement / integration mandate, early 2026
H.R. 1, “One Big Beautiful Bill Act,” signed July 4, 2025 — Medicaid work requirement provisions — KFF: Work Requirements in the 2025 Federal Budget Reconciliation Law
CBO estimate: $326 billion in Medicaid cuts over 10 years — Congress.gov: Work Requirements After P.L. 119-21; KFF Medicaid Work Requirements Tracker
NPR, June 2026 — people with serious illnesses losing Medicaid due to paperwork burden
NPR: Trump FY2026 budget — 43% cut to HUD rental assistance, Section 8 block grant proposal
Shelterforce / Capital & Main — 181,900 households (House) and 107,800 (Senate) losing vouchers
City of Grants Pass v. Johnson, 603 U.S. (2024) — anti-camping enforcement, criminalization of homelessness
IMD Exclusion, Social Security Act of 1965 — NAMI: Medicaid IMD Exclusion; Congress.gov: IMD Exclusion Overview
ABHW IMD Issue Brief, 2025 — 16 states with mental health waivers; 37 states with SUD waivers
RFK Jr. Senate confirmation statements; Manhattan Institute and AEI published case for full IMD exclusion repeal
I work for a non-profit guide dog foundation, seeing stuff like this, knowing some people out there think individuals with disabilities are less than sickens me. The clients we deal with are from all walks of life and some do get government assistance, especially if they are a veteran. What ever happened to basic common decency.
So thorough and well researched, thank you so much for your important work. This isn’t easy to understand because it’s so heartbreaking but you really help💞